


The pathogenesis of rheumatoid arthritis in radiological studies.
Part II: Imaging studies in rheumatoid arthritis
Iwona Sudoł‑Szopińska, Katarzyna Zaniewicz‑Kaniewska, Agnieszka Warczyńska, Genowefa Matuszewska, Fadhil Saied, Wojciech Kunisz
 Affiliation and address for correspondence
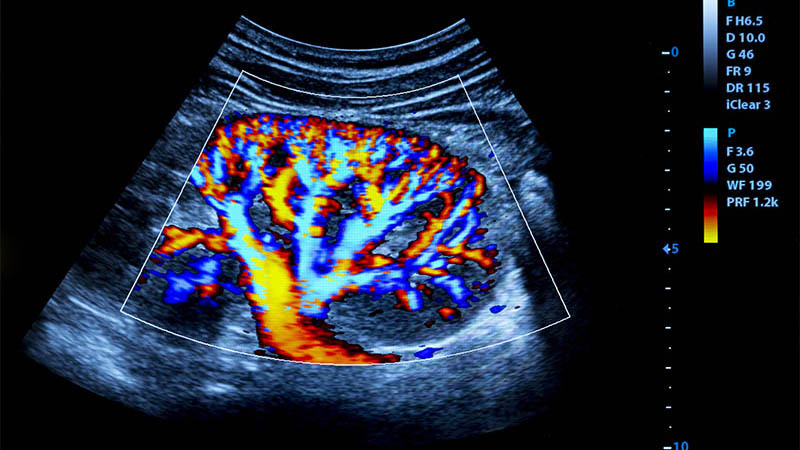
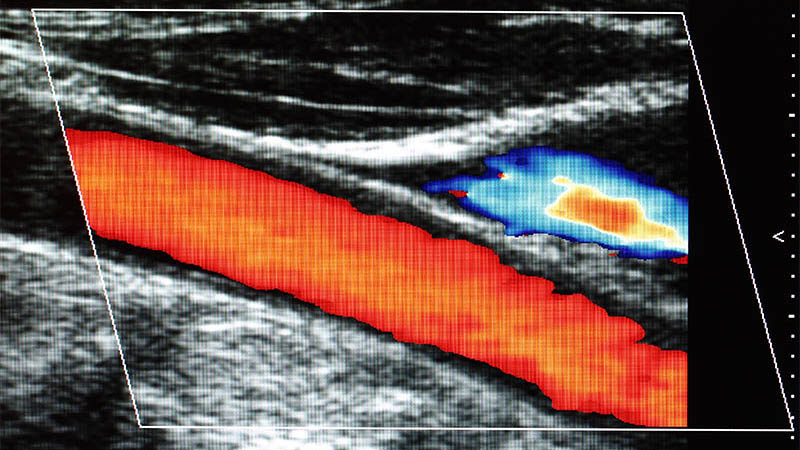
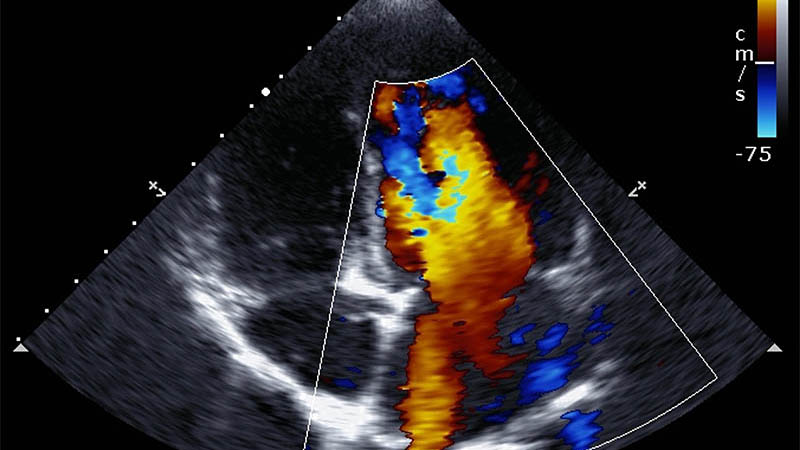
Affiliation and address for correspondenceEarly diagnosis of rheumatoid arthritis followed by early initiation of treatment, prevent the destruction of joints and progression to disability in the majority of patients. A traditional X‑ray fails to capture early inflammatory changes, while late changes (e.g. erosions) appear after a significant delay, once 20–30% of bone mass has been lost. Sonography and magnetic resonance imaging studies have shown that erosions are seen in the first 3 months from the appearance of symptoms in 10–26% of patients, while in 75% they are seen in the first 2 years of the disease. Power Doppler ultrasound and dynamic magnetic resonance studies allow for qualitative, semiquantitative and quantitative monitoring of the vascularization of the synovium. In addition, magnetic resonance enables assessment of the bone marrow. The ultrasonographic examination using a state‑of‑the‑art apparatus with a high‑frequency probe allows for images with great spatial resolution and for the visualization of soft tissues and bone surfaces. However, the changes seen in ultrasonography (synovial pathologies, the presence of exudate, tendons changes, cartilage and bone lesions, pathologies of tendon attachments and ligaments – enthesopathies) are not only specific for rheumatoid arthritis and occur in other rheumatic diseases. Qualitative methods are sufficient for diagnosing the disease through ultrasound or magnetic resonance imaging. Whereas semiquantitative and quantitative scales serve to monitor the disease course – efficacy of conservative treatment and qualification for radioisotope synovectomy or surgical synovectomy – and to assess treatment efficacy.
