


Can ultrasound be helpful in selecting optimal management methods for pregnancies complicated by placental non-trophpblastic tumors?
Nabil Abdalla, Robert Piórkowski, Paweł Stanirowski, Monika Pazura, Krzysztof Cendrowski, Włodzimierz Sawicki
 Affiliation and address for correspondence
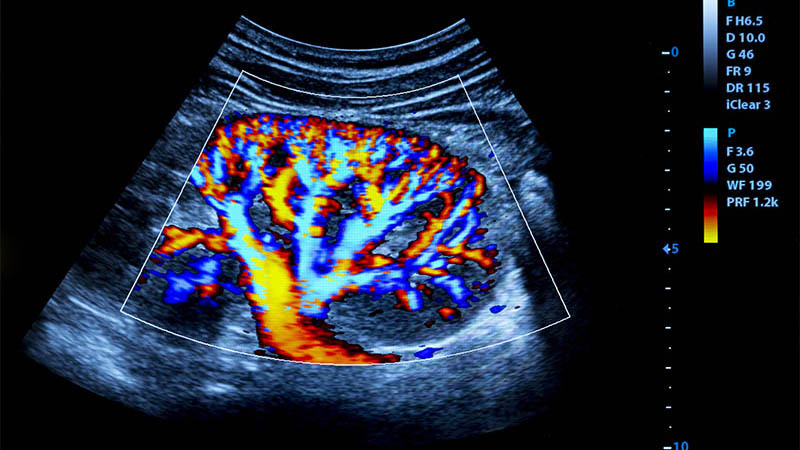
Affiliation and address for correspondencePlacental chorioangioma is the most common subtype of non-trophoblastic placental tumors. Other subtypes are very rare and usually associated with an uneventful course of pregnancy. Most chorioangiomas are small and of no clinical significance. Giant chorioangiomas may be associated with serious fetal and maternal complications. So far, no established ultrasound guidelines are available for the management of placental non-trophoblastic tumors. This may be attributed to the rarity of the disease entity and its different clinical features and complications. In this article, the role of ultrasound findings such as the tumor’s size, vascularity, feeding vessels, amniotic fluid and location of the placenta in the diagnosis, treatment and follow up of these tumors is presented relying on up-todate literature review. Conservative management with serial ultrasound examinations can be an adequate method for monitoring small uncomplicated tumors. Ultrasound-guided procedures such as amnioreduction and cordocentesis can be used for amelioration of complications. Chorioangioma-specific treatment is reserved for complicated cases in the second trimester of pregnancy when prematurity is a matter of concern. Endoscopic laser ablation is indicated when the feeding vessel is superficial and small. Interstitial laser ablation is helpful when the placenta is located in the anterior uterine wall. Ligation of the feeding vessels is preferred when they are large. Alcohol injection should be performed away from the vasculature to prevent toxicity. Microcoils should be inserted as near as possible to the tumor to prevent collateral formation. Ultrasound is also a method of choice for monitoring the effectiveness of these procedures.

